Lecture notes for Friday, March 4, 2016
Cartilage and Bone
Vertebrate skeletons are made of cartilage and bone.Bone is a composite of type I collagen (protein fibers) and calcium phosphate crystals.
Cartilage is a composite of type II collagen and chondroitin sulfate (sulfated polysaccharides) sugar chains with sulfate side groups.
Three kinds of cartilage:
-
* Hyaline cartilage: stiff and fairly strong: articular cartilages, replacement skeleton, distal ends of ribs.
* Elastic cartilage: supporting ears, larynx, tip of nose (weak and rubbery)
* Fibrous cartilage: intervertebral disks; very tough and strong: but sometimes it herniates
("slipped discs")
Cartilage is NOT vascularized; blood vessels can't penetrate into it; there are physical reasons why they can't. Nerve growth cones also can't penetrate cartilage.
And many people believe there are inhibitory substances, that repel blood vessels.
The story about sharks not getting cancer seems to be a myth; cartilage won't cure or prevent cancer.
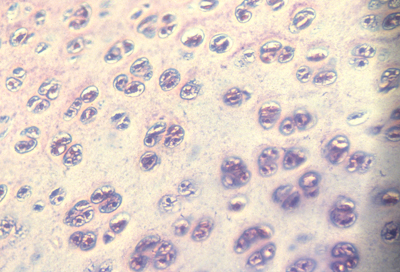
Bone is made by different kind of differentiated cell called an osteocyte; some scientists prefer to call them osteoblasts.
Osteocytes secrete collagen, but the calcium phosphate crystals are never inside the osteocytes; It is not known how they are caused.
Bone is constantly dissolved and digested by acid and enzyme secreted by a large multicellular variant kind of macrophage. These special cells are called osteoclasts.
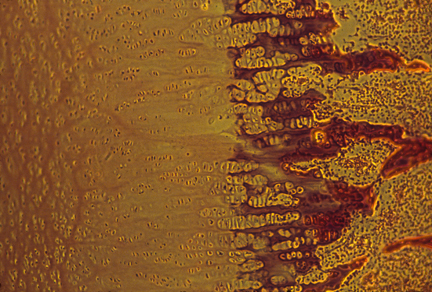
In an adult human, the skeleton is about 95% bone, but in the fetus the skeleton is about 95% cartilage. All but some bones in the skull are originally made of cartilage, which is gradually replaced by bone.
For example, your ribs are first made entirely made out of cartilage; So are your vertebrae, your humerus, radius, ulna, finger bones, etc. almost everything.
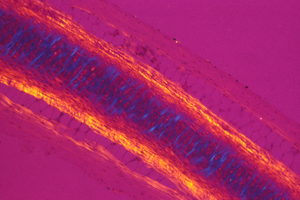
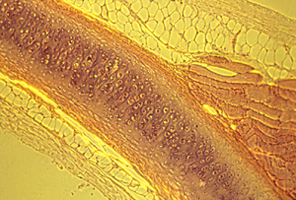
Then cartilage is destroyed a little bit at a time, and bone is formed in its shape and location. Sometimes people think and say that cartilage "changes into bone", but replacement is much closer to the truth. (Actually, some of the collagen fibers may continue to exist. That's what it looks like in some of my photographs, but I am not sure.)
The reason for this strange replacement is that bone cannot grow by internal swelling, but cartilage can.
From the late 1800s until around 1950 or 60, textbooks taught that cartilage was more primitive than bone, and had evolved before bone, and that its replacement was considered a good case of "ontogeny recapitulating phylogeny". Then it was decided that isn't true, and that bone evolved before cartilage, and that this replacement process is a method for the skeleton to grow bigger and longer by swelling.
Cartilage and Electro-Osmosis
Our joints are lined with thin layers of "articular cartilage", and many joints contain sheets of cartilage. Articular cartilage is very slippery, except where it is actually attached to bones. It feels like Teflon.Damage to articular cartilage is the reason millions of people need to have knee replacements, hip replacements, etc. Sometimes cartilage gets physically damaged; sometimes it gets attacked by the immune system. Without it, bones will rub directly against each other, and there is terrible pain. If you could repair articular cartilages, for example by colonizing joints with enough new cartilage cells, that would save much suffering and expense. Progress has been made in this direction. Cartilage cells (chondrocytes) survive, grow and divide well in tissue culture. They are the only cell type I know that doesn't need vascularization; they tolerate low concentrations of oxygen. Articular cartilages are made of the sub-type known as hyaline cartilage.
Our external ears and the tips of our noses are supported by a special version of cartilage, called elastic cartilage. This contains more elastin fibers, and fewer collagen fibers, than either hyaline or fibrous cartilage. Physically, elastic cartilage is much less stiff; it also springs back to its original shape quicker.
The flat blocks of cartilage between the central parts of your backbone are made of fibrous cartilage. These are strongly attached to the bone on both sides: they are sort of the opposite of lubrication.
A so-called "slipped disk" is a herniation of the collagen layer that surrounds each intervertebral disk. Mechanically, it isn't at all analogous to a coin slipping out of a pile of coins (as suggested by "slipped").
Medically, it would be a huge step forward if someone invented a way to cause the surface tissues of these disks to contract and pull the herniation back in, and heal the "slip". No research is being done in that direction, as best I know. One reason is that the physics of cartilage is not correctly understood by most physicians and biologists. They never learned about electro-osmosis.
----------
The shape, strength and elasticity of every cartilage is caused by a counter-balance of two forces:
One force is electro-osmotic swelling, caused by water being drawn inward by osmotic forces.
The other force is elastic stretching of collagen fibers (and sometimes also elastin fibers).
(Some of these collagen fibers run through the interior of cartilages; other collagen fibers are wrapped around the outside of cartilages. The interior ones are more important in articular cartilage. The surface wrapping ones are most important in inter-vertebral disks (The "annulus fibrosis", which surrounds the "nucleus pulposis". What nifty old names; both from Latin.)
The kind of osmosis that you already know about depends on having a semi-permeable membrane that surrounds some water in which either molecules or ions are dissolved. The membrane needs to allow water to diffuse through it, but not allow the dissolved ions or molecules to diffuse through it. The third requirement is for a higher concentration of ions or molecules inside the surrounding membrane, as compared with their concentration outside the membrane. Water will then exert a surprisingly strong force diffusing toward wherever the concentration of dissolved ions or molecules are higher. This force obeys the ideal gas law (strange to say!), good old PV=nRT.
You remember that one from high school chemistry, right? If you put two grams of hydrogen in a one liter flask, it will push outward with a force of twenty two atmospheres. Eighteen grams of oxygen, ditto. A one molar solution of glucose dissolved in one liter of water, can produce 22 atmospheres of osmotic pressure. Please understand that osmosis is an entropic effect; it doesn't depend on attraction forces between water and dissolved materials, so long as they are soluble in water. Diffusing units per volume.
Suppose you had some other method able to confine diffusing ions to a certain limited volume? That could give you an osmotic pressure, proportional in strength to the concentration of ions whose diffusion is restricted. This pressure would push against whatever restricts the diffusion of the ions. Inside cartilage, there are many sulfate groups covalently bound to chains of sugars, which are bound to fibrous proteins.
Hydrogen ions, sodium ions and other cations are free to diffuse around amongst the sulfates, but are not free to leave their vicinity. Negative charges on the sulfates hold positive ions near them. Water tends to dilute the diffusing cations, producing an osmotic pressure equal to the cation's molar concentration. (times R, the gas constant, times T the Kelvin temperature, divided by volume).
The electric field serves the role of the semi-permeable membrane. So the force pulls on the sulfates.
You probably won't find this mentioned if you look up the meaning of electro-osmosis. And you probably won't find electro-osmosis mentioned in books about cartilage, or about back surgery or knee replacement.
If you squeeze a piece of cartilage, you can produce hundreds of volts (but a tiny amperage). Pressure squeezes out some of the water, which carries cations with it, producing a momentary voltage (positive outside, negative inside); then when you release the pressure, a brief but high voltage is generated in the opposite direction. These voltages are much bigger, and equally brief, as whatever piezo-electric voltages are produced by squeezing or twisting bones (a phenomenon which gets very much more attention.
Suppose you impose an electric voltage (using wires and electrodes, batteries, rectifiers, etc. a regular electric voltage) oriented somewhat parallel to the surface of a piece of cartilage,, what will happen? The same will happen if you create a voltage along the surface of a piece of glass, incidentally. Water flows toward the negative electrode. That is because of the slightly greater concentration of positive ions in the water next to the negatively charged immobile material. The same flow occurs if a voltage is imposed through pores of a piece of clay or glass, or cartilage.
This voltage-induced flow of water is what most people call electro-osmosis. (Those few people who have ever heard of it at all.) In your opinion, is one or the other definition of electro-osmosis correct, and the other meaning is incorrect? Or are these two sides of the same coin? You can't get one without the other?
Two results of the same set of causes?
How might knowledge of this subject help surgeons repair knees or slipped disks?
NPR link to news story mentioned in the lecture, about the astronaut who just returned from nearly a year in space and was a couple of inches taller than before he left earth.
What happened was expansion of cartilage in the intervertebral disks and perhaps also at the ends of the leg bones.
----------
From the lecture on forces:
Can the flat shape of an ear cartilage be caused by concentrating synthesis of cartilage in certain directions?
Answer: No, because osmotic pressure is a scalar, its strength can't vary with direction; But directional differences in tension can occur.
Because electro-osmotic pressure of cartilage is a scalar, it cannot possibly vary with direction. Pressure can vary from one location to another; and that can contribute to shape; but directional expansion has to be mostly caused by weakening of tension in one axis relative to tensions in the perpendicular axes.